
Best Peptides for Weight Loss During Perimenopause: What the Evidence Says
An evidence-based guide to GLP-1s, growth hormone peptides, and what actually works for midlife weight gain.

Key Takeaways
- Tirzepatide and semaglutide (GLP-1 receptor agonists) have the strongest clinical evidence for perimenopause weight loss.
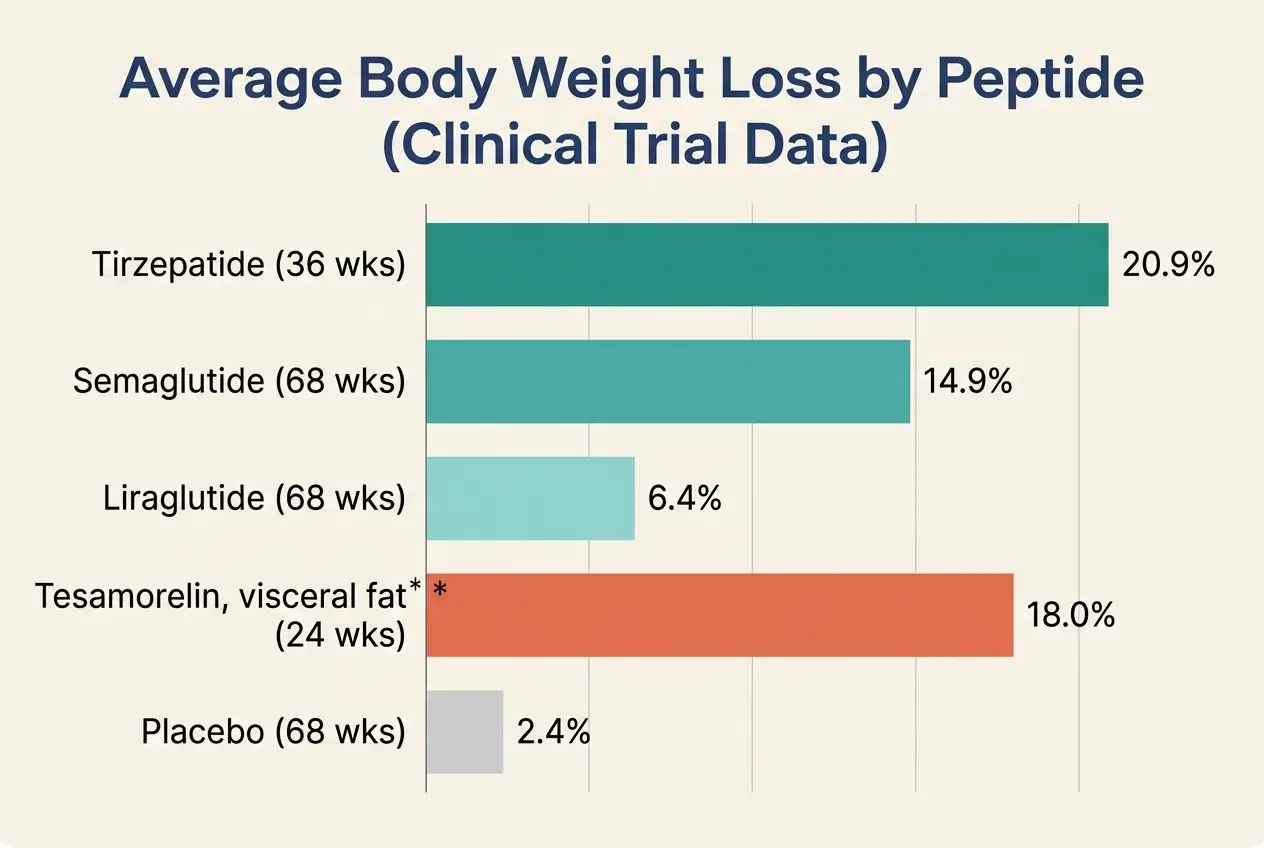
- Tirzepatide produced 20.9% average body weight reduction in clinical trials, outperforming semaglutide and liraglutide.
- Growth hormone peptides like tesamorelin target visceral belly fat and help preserve lean muscle during weight loss.
- Combining GLP-1 therapy with hormone replacement therapy may boost weight loss results by 35% based on 2026 Mayo Clinic research.
- 72% of GLP-1 users stop within two years, and regained weight returns mostly as fat, making strength training and protein intake non-negotiable.
- All peptide therapy requires baseline labs, medical supervision, and a qualified provider experienced in perimenopause.
The best peptides for weight loss during perimenopause fall into two main categories. FDA-approved GLP-1 receptor agonists, including tirzepatide and semaglutide, carry the strongest clinical evidence, with tirzepatide producing up to 20.9% body weight reduction in trials [1].
Growth hormone secretagogues like tesamorelin and ipamorelin/CJC-1295 offer additional benefits for body composition and muscle preservation.
A 2026 Mayo Clinic study found that combining GLP-1 therapy with hormone replacement therapy produced 35% greater weight loss in postmenopausal women [2].
All peptide therapy requires medical supervision.
Peptides for Perimenopause Weight Loss at a Glance
| Peptide | Category | FDA Status | Mechanism | Weight Loss | Perimenopause Benefit | Key Risk | Monthly Cost | Administration |
|---|---|---|---|---|---|---|---|---|
| Tirzepatide (Zepbound) | GLP-1 + GIP dual agonist | FDA Approved | Appetite suppression, insulin sensitivity, fat metabolism | 15-21% body weight | Addresses insulin resistance and visceral fat | GI side effects (nausea, diarrhea) | $199-$1,399 | Weekly injection |
| Semaglutide (Wegovy) | GLP-1 agonist | FDA Approved | Appetite suppression, slower gastric emptying | 14.9% body weight | Most accessible; oral option available | GI side effects (lower than tirzepatide) | $99-$650 | Weekly injection or oral |
| Liraglutide (Saxenda) | GLP-1 agonist | FDA Approved | Appetite suppression | 5-8% body weight | Alternative for those intolerant to others | Daily injection; less effective | $200-$500 | Daily injection |
| Tesamorelin | GH secretagogue (GHRH analog) | Off-Label | Stimulates GH release; targets visceral fat | 9-18% visceral fat reduction | Targets visceral belly fat; preserves muscle | Cancer risk for GH-sensitive individuals | $300-$600 | Daily injection |
| CJC-1295 + Ipamorelin | GH secretagogue combo | Not Approved | Sustained + acute GH release | Moderate (limited data) | Body composition, sleep, recovery | IGF-1 elevation; cancer concern | $200-$500 | Daily injection (often cycled) |
| Sermorelin | GH secretagogue (GHRH analog) | Not Approved | Stimulates natural GH production | Mild to moderate | Sleep quality, gentle GH support | Minimal; well-tolerated | $150-$400 | Daily injection |
| BPC-157 | Tissue repair peptide | Not Approved | Anti-inflammatory, gut healing | No direct weight loss | May support exercise recovery and gut health | Pro-angiogenic (theoretical cancer concern) | $100-$300 | Injection or oral |
| AOD-9604 | Modified HGH fragment | Not Approved | Fat metabolism stimulation | Limited human data | Targeted fat reduction (theoretical) | Limited safety data | $150-$350 | Injection |
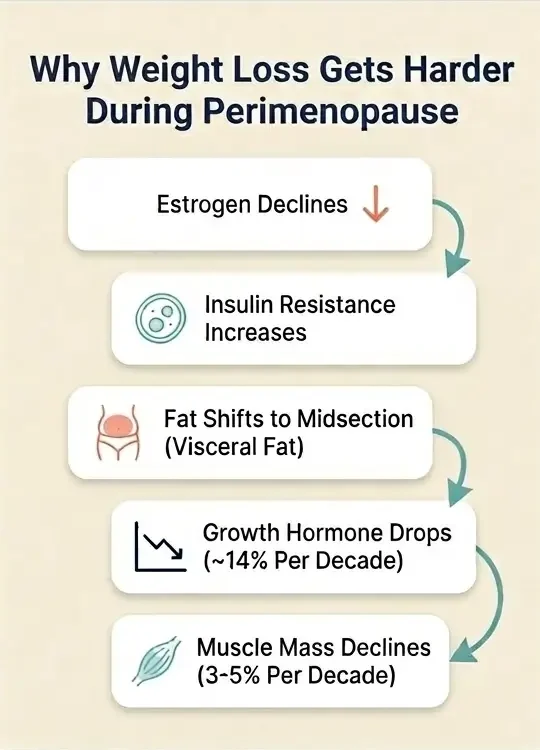
Why Perimenopause Makes Weight Loss So Difficult
You are not imagining it. Perimenopause changes how your body stores fat, burns calories, and responds to exercise.
Understanding these changes explains why your usual approach stopped working and why peptides have become so appealing for women in this phase.
Estrogen decline drives the most visible shift. As estrogen levels fluctuate and eventually drop during perimenopause (typically between ages 40-55), your cells become less responsive to insulin [8].
Insulin resistance means your body converts more calories into stored fat rather than available energy. This fat preferentially accumulates around your midsection as visceral fat, the deep abdominal fat that wraps around internal organs and raises your risk for cardiovascular disease and type 2 diabetes [9].
Simultaneously, progesterone drops faster than estrogen during early perimenopause.
Lower progesterone elevates cortisol, your primary stress hormone. Elevated cortisol promotes additional visceral fat storage and makes your body more likely to break down muscle for energy [10].
Growth hormone (GH) production also declines with age, dropping roughly 14% per decade after age 30 [11].
GH plays a direct role in fat metabolism and muscle maintenance. Without adequate GH, your body loses lean muscle mass at a rate of approximately 3-5% per decade, and this process accelerates during perimenopause [12].
Less muscle means a slower resting metabolic rate, which means you burn fewer calories doing nothing.
“So why can’t I just eat less and exercise more?”
You can try. But calorie restriction during perimenopause often triggers additional cortisol release, which worsens insulin resistance, accelerates muscle loss, and signals your body to hold onto fat stores even more aggressively. This creates a cycle where conventional dieting makes the hormonal problem worse, not better [13].
Peptide therapy targets these specific metabolic disruptions rather than simply restricting calories. The next section explains how different peptide categories address different parts of this problem.
What Peptides Are and How They Work for Weight Loss
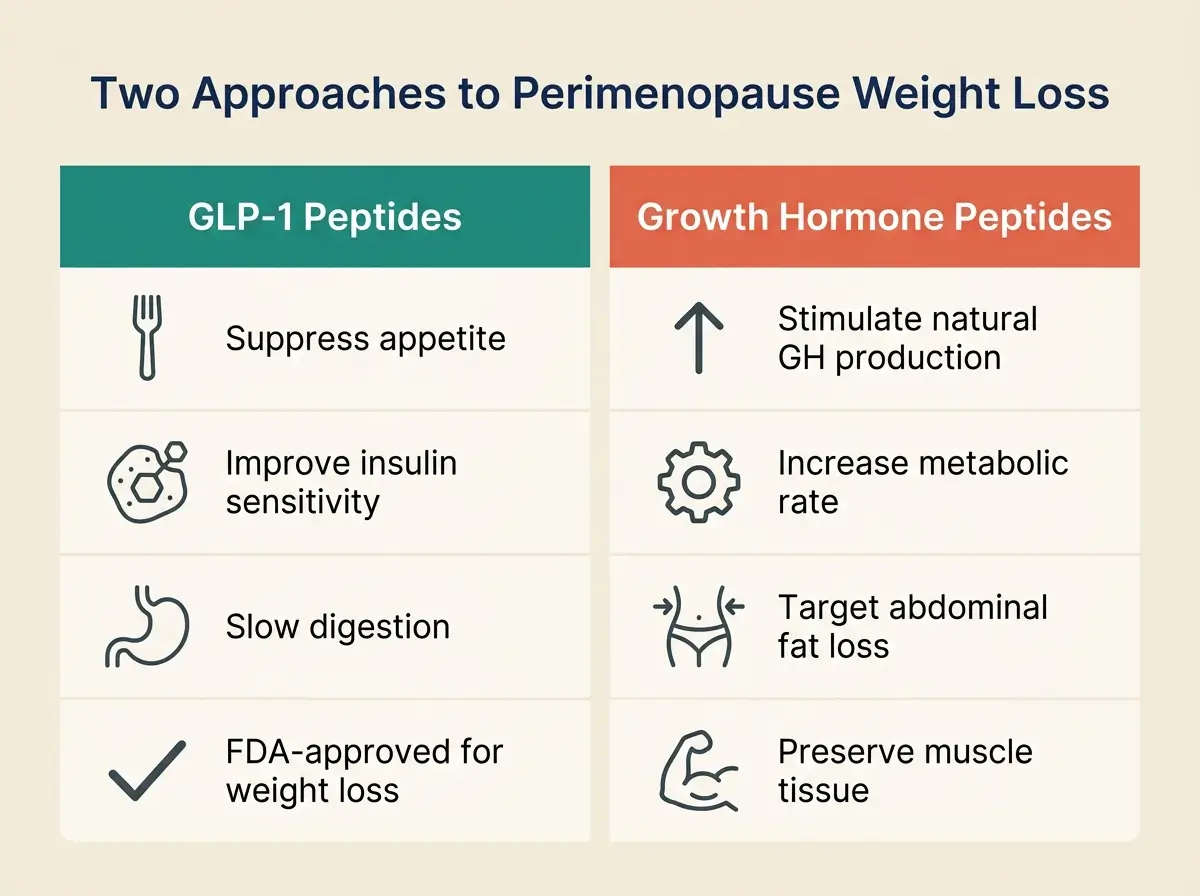
GLP-1 Receptor Agonists
Mimic a gut hormone to reduce appetite, improve insulin sensitivity, and slow digestion. Strongest clinical evidence for weight loss.
ExamplesTirzepatide, Semaglutide, Liraglutide
Growth Hormone Secretagogues
Signal your pituitary gland to produce more growth hormone for fat metabolism and muscle preservation.
ExamplesTesamorelin, CJC-1295 + Ipamorelin, Sermorelin
Support and Repair Peptides
Reduce inflammation, heal gut lining, and support recovery. Indirect weight management support.
ExamplesBPC-157, GHK-Cu, NAD+
Peptides are short chains of amino acids (the building blocks of protein) that act as signaling molecules in your body.
Each peptide delivers a specific instruction to your cells, such as “release growth hormone,” “slow digestion,” or “repair this tissue” [14].
Your body produces thousands of natural peptides. Therapeutic peptides are synthetic versions designed to mimic or amplify these natural signals. When it comes to peptide therapy for women in perimenopause, three categories matter most.
- GLP-1 receptor agonists mimic a gut hormone called glucagon-like peptide-1. They reduce appetite, slow stomach emptying so you feel full longer, and improve your cells’ response to insulin [15]. Tirzepatide and semaglutide fall into this category. These are the ONLY peptides currently FDA-approved for weight loss in adults.
- Growth hormone secretagogues signal your pituitary gland to produce more growth hormone. Higher GH levels promote fat metabolism (particularly visceral fat), preserve lean muscle, and support recovery and sleep [16]. Tesamorelin, CJC-1295, ipamorelin, and sermorelin fall into this group.
- Tissue repair and support peptides like BPC-157 don’t cause weight loss directly. They reduce inflammation, support gut healing, and improve recovery from exercise. These may help you stay consistent with the physical activity that supports weight management during perimenopause.
The Best GLP-1 Peptides for Perimenopause Weight Loss
GLP-1 receptor agonists have the most robust clinical evidence for weight loss of any peptide category. They directly address two of the biggest metabolic problems of perimenopause, insulin resistance and appetite dysregulation, which is why they’ve become the first-line medical option.
Tirzepatide: Most Effective
Tirzepatide (brand names Zepbound for weight loss, Mounjaro for type 2 diabetes) activates two receptors simultaneously, GLP-1 and GIP (glucose-dependent insulinotropic polypeptide). This dual action makes it the most potent weight loss peptide available today.
The numbers are significant. In a 2024 clinical study of 670 adults with overweight or obesity, participants taking tirzepatide achieved an average 20.9% reduction in body weight at 36 weeks [1].
Participants who stopped the medication regained 14% of their body weight, while those who continued lost an additional 5.5% [1].
In a head-to-head comparison, tirzepatide consistently outperforms semaglutide. A 2021 New England Journal of Medicine trial of 1,973 patients found that all three tirzepatide dose groups lost 4-12 more pounds than the semaglutide group over 40 weeks [3].
A larger 2024 JAMA Internal Medicine cohort study of 18,386 patients confirmed that tirzepatide produced significantly greater weight loss than semaglutide [17].
For perimenopausal women specifically, tirzepatide’s ability to improve insulin sensitivity addresses a root cause of midlife weight gain, not just a symptom. You receive it as a once-weekly injection, starting at 2.5 mg and gradually increasing to 5, 10, or 15 mg over several weeks [18].
The most common side effects are gastrointestinal, including nausea, diarrhea, and vomiting. These occur at a 2-5% higher rate than with semaglutide and typically improve as your body adjusts to the medication. Starting at a low dose and increasing gradually helps minimize these effects. [3]
Cost varies widely. Through telehealth platforms, you can expect to pay $199-$1,399 per month depending on dose and provider.
Semaglutide: Most Accessible
Semaglutide (Wegovy for weight loss, Ozempic for type 2 diabetes) activates GLP-1 receptors to suppress appetite, slow gastric emptying, and improve insulin function.
A landmark 2021 study of 1,961 adults in the New England Journal of Medicine found that participants receiving 2.4 mg semaglutide weekly lost an average of 14.9% of their body weight over 68 weeks, compared to 2.4% in the placebo group [4].
Of those taking semaglutide, 86.4% achieved at least 5% weight loss, and 50.5% achieved at least 15% [4].
When compared to liraglutide (another GLP-1), semaglutide produced 15.8% body weight reduction versus 6.4% for liraglutide over 68 weeks [19].
Semaglutide’s biggest advantage for perimenopausal women is accessibility. At least 10 reputable telehealth platforms carry it [20]. Eight of those offer oral formulations, which may appeal to you if injections are a barrier [20].
The oral version delivers lower bioavailability than the injectable form (under 2% vs up to 50% for injections), so the injectable remains the clinical standard. [21][22]
Side effects are similar to tirzepatide but slightly less common, with up to 5% lower rates of nausea [3]. Monthly costs range from $99 (starting oral dose) to $650 through telehealth providers.
Liraglutide: The Third Option
Liraglutide (Saxenda for weight loss) was the first GLP-1 to receive FDA approval for obesity treatment in 2014. It works through the same mechanism as semaglutide but requires daily injection rather than weekly.
Multiple meta-analyses confirm it is less effective than both tirzepatide and semaglutide for weight loss [5]. You may consider it if you cannot tolerate the other two options, though for most perimenopausal women seeking maximum impact, tirzepatide or semaglutide will be the stronger choice.
While GLP-1 receptor agonists produce the most dramatic weight reduction, they primarily work through appetite and insulin pathways. Growth hormone peptides offer a different approach, one that targets body composition directly by addressing the muscle-preserving, fat-metabolizing functions that decline during perimenopause.
Growth Hormone Peptides: Targeting Body Composition During Perimenopause
Growth hormone (GH) peptides appeal to perimenopausal women for a specific reason. They aim to improve body composition, meaning less visceral fat and more preserved lean muscle, rather than just reducing the number on the scale.
This matters because losing weight during perimenopause without preserving muscle can leave you with a worse metabolic profile than before.
Tesamorelin: Best Non-GLP-1 Option
Tesamorelin is a synthetic analog (a lab-made version) of growth hormone-releasing hormone (GHRH). It tells your pituitary gland to produce more GH, which then stimulates fat breakdown, particularly in the visceral compartment.
The FDA approved tesamorelin for HIV-associated lipodystrophy (excess abdominal fat from antiretroviral treatment). In that population, a 2010 clinical trial showed an average 18% decrease in visceral fat compared to placebo [6].
A 2006 study of GH-deficient Japanese adults receiving growth hormone replacement showed 9.3% body fat reduction at 24 weeks, supporting the fat-reducing potential of GH-pathway stimulation [7].
A 2019 study found tesamorelin also increased skeletal muscle area and density [23].
For perimenopausal women, this profile is particularly relevant. Tesamorelin targets the exact type of fat (visceral, abdominal) that accumulates during perimenopause, while simultaneously helping preserve the muscle you’re naturally losing.
The weight loss is more moderate than with GLP-1s, but the body composition change may be more favorable.
The trade-off is convenience. Tesamorelin typically requires daily injections (5-7 per week), versus once-weekly for tirzepatide. It is less available through telehealth and costs $300-$600 per month.
CJC-1295 + Ipamorelin
This combination is popular in wellness and anti-aging circles. CJC-1295, a GHRH analog, provides sustained GH elevation over several days.
A 2006 study published in the Journal of Clinical Endocrinology & Metabolism showed it increased mean GH concentrations by 2-10x for 6+ days after a single injection [24].
Ipamorelin selectively stimulates GH release without raising cortisol or ACTH [25], an advantage for perimenopausal women already dealing with elevated stress hormones.
Together, these peptides can improve body composition, sleep quality, recovery time, and skin health.
(Ed. note: “improve” here means within the context of clinical observation and small studies, not large-scale randomized controlled trials.)
However, you need to understand what “not FDA-approved” means in practice. Neither CJC-1295 nor ipamorelin has completed the rigorous safety testing required for FDA approval.
The relationship between elevated IGF-1 (insulin-like growth factor-1, which increases with growth hormone stimulation) and cancer risk is documented in the medical literature.
A review in Proceedings of the National Academy of Sciences found positive associations between high circulating IGF-1 levels and risk for breast, colorectal, and other cancers [26].
Women with a personal or family history of hormone-sensitive cancers should avoid these peptides until more safety data becomes available.
Sermorelin
Sermorelin is a milder GHRH analog that stimulates natural GH production. It’s often considered the most conservative entry point for GH peptide therapy. Women report improvements in sleep quality, energy, body composition, and skin texture. It works by supporting your body’s existing GH pathways rather than overriding them.
Sermorelin is not FDA-approved for weight loss but has a generally favorable safety profile when prescribed by a qualified provider. Monthly costs range from $150-$400.
You may now be wondering about other peptides you’ve seen mentioned in online forums and wellness blogs. Some of these play a supporting role, but none should be your primary weight loss tool.
What About BPC-157, AOD-9604, and Other Peptides?
Several peptides frequently appear in conversations about perimenopause and weight loss. While they may offer complementary benefits, none of them have strong clinical evidence for direct weight reduction.
- BPC-157 (Body Protection Compound-157) is a synthetic peptide derived from a protein in human gastric juice. Animal studies show impressive results for gut healing, joint repair, and inflammation reduction [27].
For perimenopausal women dealing with joint pain, gut issues, or exercise-related injuries, BPC-157 could theoretically support consistent physical activity, which indirectly supports weight management.
The FDA classified BPC-157 as a Category 2 bulk drug substance in 2023, meaning it lacks sufficient evidence of human safety for commercial compounding [28].
No human trials have evaluated it for weight loss. Its pro-angiogenic properties (promoting blood vessel formation) also raise theoretical concerns about tumor growth [29].
- AOD-9604 is a modified fragment of human growth hormone designed to isolate fat-burning properties. While the concept is promising, human clinical data remains limited and it is not FDA-approved.
- NAD+ supports cellular energy production and may help with perimenopause-related brain fog and fatigue. It does not directly cause weight loss.
- GHK-Cu is a copper peptide with documented skin benefits, including a study showing 55.8% reduction in wrinkle volume in women aged 40-65 using topical application [30].
Relevant to overall perimenopause wellness but not a weight loss tool.
The bottom line on these peptides is straightforward. They may complement a weight loss strategy that’s built around GLP-1s, growth hormone peptides, or both. They should not be the foundation of your approach.
If your provider recommends any of these supportive peptides as part of a broader protocol, sourcing from a verified supplier is non-negotiable.
Apollo Peptide Sciences carries BPC-157, CJC-1295/Ipamorelin, GHK-Cu, and NAD+ with published third-party lab testing on every product. Their catalog includes Certificates of Analysis so you can verify purity before use.
Recent research has added another powerful variable to this equation, the interaction between hormone replacement therapy and peptide-based weight loss.
The HRT + Peptide Connection: Emerging Evidence
If you’re considering both hormone replacement therapy (HRT) and peptide therapy for perimenopause, a growing body of research suggests these approaches may work better together than either does alone.
A January 2026 study led by Mayo Clinic and published in The Lancet Obstetrics, Gynaecology, & Women’s Health analyzed 120 postmenopausal women with overweight or obesity who received tirzepatide for 12 or more months. Women who also received menopausal hormone therapy lost 35% more weight than those taking tirzepatide alone [2].
“In this observational study, women who used menopausal hormone therapy lost about 35% more weight than women taking tirzepatide alone,” said Dr. Maria Daniela Hurtado Andrade, endocrinologist at Mayo Clinic and senior author of the study [2].
The researchers noted that preclinical data suggest estrogen may enhance the appetite-suppressing effects of GLP-1 [2]. Earlier data presented at the Endocrine Society’s 2025 annual meeting showed similar trends. The combination group achieved 17% total body weight loss compared to lower results in the non-HRT group [31].
These findings carry a significant caveat. The Mayo Clinic study was observational, not a randomized controlled trial. Women using HRT may have also been more engaged in healthier behaviors, or their HRT may have improved sleep and quality of life in ways that supported weight loss independently [2].
The researchers plan to test these observations in a randomized clinical trial [2].
For practical purposes, this data suggests something you should discuss with your provider. If you’re already taking or considering HRT for perimenopause symptoms like hot flashes, night sweats, or mood changes, you may see an added weight loss benefit when combining it with a GLP-1 peptide.
This is an active area of research that will likely yield clearer answers in the next 1-2 years.
You should also understand what happens after you stop peptide therapy, because discontinuation is common and the consequences are particularly relevant during perimenopause.
35%
more weight lost when combining tirzepatide with hormone replacement therapy
Mayo Clinic / The Lancet, January 2026
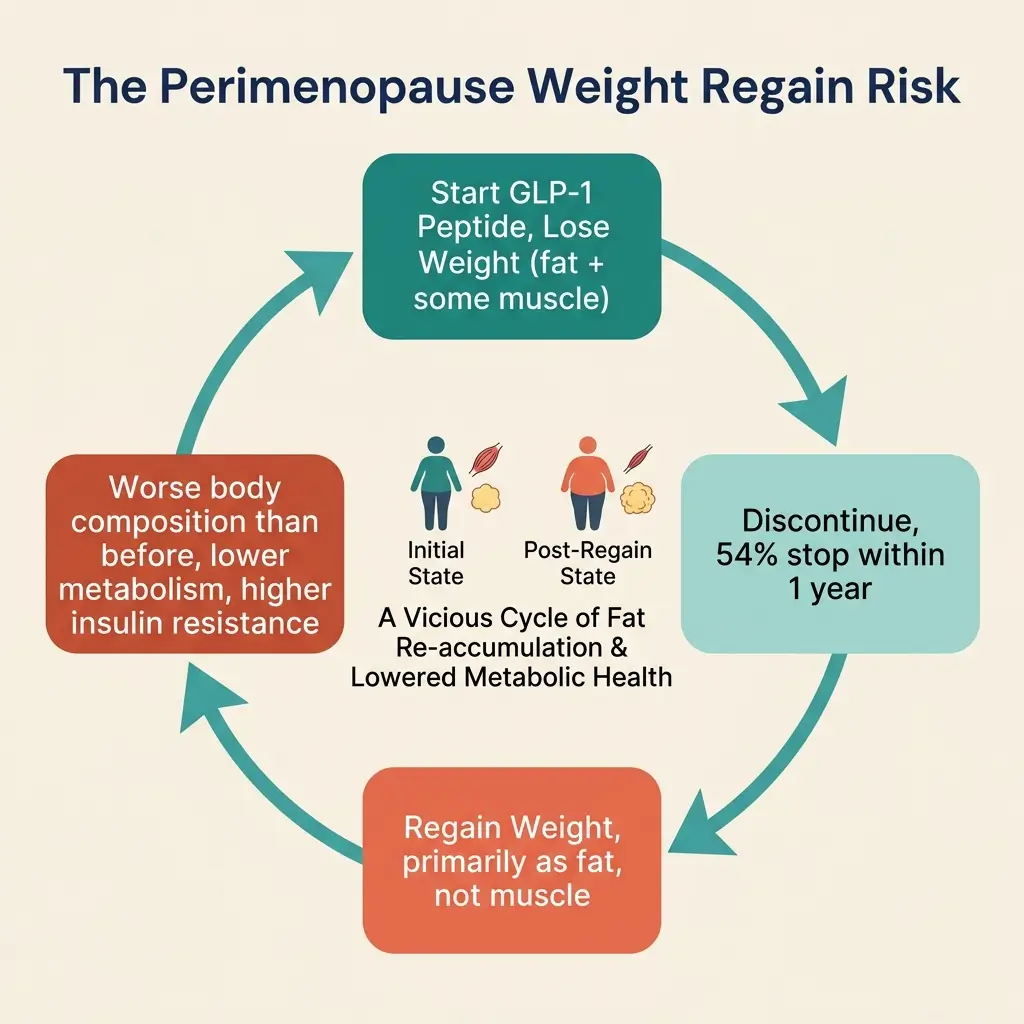
What Happens When You Stop?
Most people do not stay on GLP-1 medications indefinitely. A 2025 analysis found that 54% of GLP-1 users discontinue within one year, and 72% stop within two years [32].
The reasons vary, including cost, side effects, achieving a target weight, or losing insurance coverage.
The weight regain pattern after discontinuation is significant. In the tirzepatide trial, participants who switched to placebo after 36 weeks regained 14% of their body weight [1].
And the weight that comes back is primarily fat mass, not muscle [33]. RAND Corporation researchers specifically highlighted this concern for perimenopausal women, who already face natural declines in muscle mass and bone density [33].
“Why does this matter more during perimenopause than at other times?”
Because you’re fighting a two-front battle. Your body is naturally shifting toward more fat and less muscle due to hormonal changes.
If you lose weight with a GLP-1, stop the medication, and regain that weight as fat while not recovering the muscle, your body composition is WORSE than before you started.
Your metabolic rate drops further. Your insulin resistance may worsen. The cycle becomes harder to break.
RAND researchers also identified the psychosocial dimensions. Weight regain after dramatic loss during perimenopause converges with mood changes, declining body satisfaction, and self-esteem challenges that are already common during this life phase. The combination can trigger anxiety, depression, and disordered eating behaviors [33][34].
Practical strategies to reduce these risks include maintaining consistent strength training during AND after peptide therapy, consuming adequate protein (aim for 1.2-1.6 grams per kilogram of body weight daily), working with your provider on gradual dose reduction rather than abrupt cessation when appropriate, and treating peptide therapy as one component of a sustainable long-term plan rather than a temporary fix.
Safety during perimenopause involves additional considerations beyond what applies to the general population.
Safety, Side Effects, and Who Should Avoid Peptides
FDA-approved GLP-1 peptides (tirzepatide, semaglutide, liraglutide) carry well-documented safety profiles from large clinical trials.
The most common side effects are gastrointestinal, including nausea, diarrhea, vomiting, and constipation [3][4].
These are typically dose-dependent and improve as your body adjusts. Starting at a low dose and increasing slowly helps manage them.
Growth hormone secretagogues (tesamorelin, CJC-1295, ipamorelin, sermorelin) may cause flu-like symptoms, fatigue, headache, and joint or muscle pain [35].
The more significant concern with GH peptides is the link between elevated IGF-1 and cancer risk. Multiple epidemiological studies associate higher circulating IGF-1 levels with increased risk for breast, colorectal, and other cancers [26].
If you have a personal or family history of hormone-sensitive cancers, growth hormone peptides should be considered contraindicated until better safety data exists.
Perimenopause adds several safety layers that your provider should address.
- Bone density. GLP-1s reduce overall body mass, including the mechanical load on your skeleton. If you already have low bone density or osteopenia (early-stage bone thinning), monitor your DEXA (bone density) scans during treatment. Strength training provides a protective stimulus.
- Muscle preservation. Pair GLP-1 therapy with resistance training and high protein intake. Some providers combine GLP-1s with GH peptides specifically to offset muscle loss during weight reduction.
- Pregnancy. Perimenopause does NOT mean you cannot get pregnant. Ovulation can still occur during irregular cycles. The FDA recommends stopping Wegovy (semaglutide) at least 2 months before a planned pregnancy [36]. Zepbound (tirzepatide) users should add barrier contraception for 4 weeks after each dose increase [18]. This is a real and frequently overlooked consideration.
- Thyroid. Both semaglutide and tirzepatide carry boxed warnings about medullary thyroid carcinoma risk, based on animal studies [4][18]. Women with a personal or family history of medullary thyroid cancer or multiple endocrine neoplasia type 2 (MEN2) should not use these medications.
- Medical-grade sourcing. Research-grade peptides sold online without a prescription can lack purity and safety verification. Only use pharmaceutical-grade peptides prescribed by a licensed provider for FDA-approved medications. For research peptides like CJC-1295/Ipamorelin or BPC-157, purity verification matters. Suppliers like Apollo Peptide Sciences publish independent third-party lab reports, Certificates of Analysis, and endotoxin testing results for every batch. Their products consistently meet or exceed 98% purity by HPLC analysis. This level of transparency is the minimum standard you should expect from any peptide supplier. The FDA has warned about counterfeit GLP-1 products that may contain incorrect doses or harmful ingredients [37].
How to Get Started
Before starting any peptide therapy for perimenopause weight loss, work through these steps with a qualified healthcare provider.
Get Baseline Labs
Request a full hormone panel (estradiol, progesterone, FSH (follicle-stimulating hormone), testosterone, DHEA-S), thyroid panel (TSH, free T3, free T4), metabolic markers (fasting glucose, fasting insulin, HbA1c (a 3-month blood sugar average)), liver and kidney function tests, and a DEXA scan for bone density. These results help your provider select the right peptide, identify contraindications, and establish benchmarks for tracking progress.
Build Your Foundation
Optimize sleep (7-8 hours), establish a strength training routine (minimum 2-3 sessions per week), increase protein intake to 1.2-1.6g per kilogram of body weight, and address chronic stress. A board-certified physician specializing in perimenopause should evaluate and treat nutritional deficiencies in vitamin D, B12, magnesium, and iron before adding peptides [38].
Discuss HRT
If you have perimenopause symptoms (hot flashes, night sweats, mood changes, sleep disruption), HRT may relieve those symptoms AND enhance your weight loss response to GLP-1 therapy based on the emerging evidence discussed earlier in this guide.
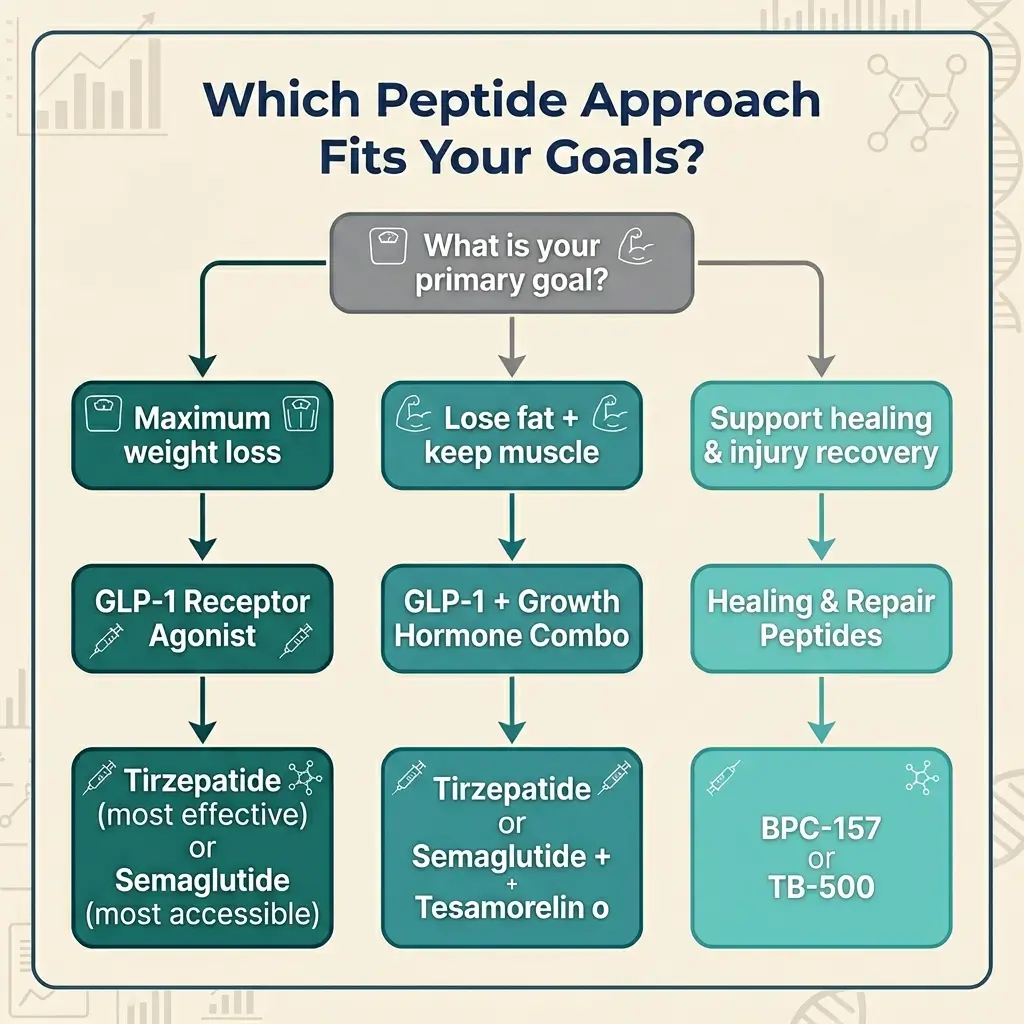
Choose Your Peptide Approach
If maximum weight loss is your priority, start with a GLP-1 receptor agonist. Tirzepatide is the most effective; semaglutide is the most accessible. If body composition matters more than total pounds lost, discuss combining a GLP-1 with a growth hormone peptide like tesamorelin. If you prefer a moderate, lower-intervention approach, sermorelin or tesamorelin alone may suit you better. For research peptides like CJC-1295/Ipamorelin, BPC-157, or GHK-Cu, look for suppliers with independent third-party testing and published COAs. Apollo Peptide Sciences meets these standards and offers free shipping on orders over $200. For FDA-approved GLP-1 medications, work with a licensed prescribing provider or telehealth platform.
Find the Right Provider
Look for a board-certified physician experienced in BOTH perimenopause management and peptide therapy. Avoid providers who prescribe without lab work or a thorough medical history review. If your consultation takes 5 minutes and involves no labs, find someone else.
Monitor and Adjust
Schedule regular follow-ups (every 4-8 weeks initially). Track your body composition (not just weight), energy levels, sleep quality, mood, and any side effects. Your provider should repeat labs every 3-6 months and adjust your protocol based on results.
Plan for the Long Term
Peptides are tools that work within a broader health strategy. The strength training, protein intake, stress management, and sleep habits you build alongside peptide therapy are what sustain your results if and when you discontinue the medication.
Regardless of which peptide category you choose, product quality directly affects your results and safety. For research peptides like CJC-1295/Ipamorelin, BPC-157, or GHK-Cu, look for suppliers with independent third-party testing and published COAs. Apollo Peptide Sciences meets these standards and offers free shipping on orders over $200. For FDA-approved GLP-1 medications like tirzepatide and semaglutide, work with a licensed prescribing provider or telehealth platform.
How We Researched This
To help you find the best peptides for weight loss during perimenopause, we reviewed over 40 sources for this guide, including:
- randomized controlled trials published in the New England Journal of Medicine, The Lancet, and JAMA Internal Medicine;
- survey data from the RAND American Life Panel;
- FDA prescribing information and safety communications; and
- expert commentary from institutions including Mayo Clinic, the Endocrine Society, and the RAND Corporation.
- We also analyzed the content and structure of 10+ competing articles ranking for related search queries to identify information gaps.
- Our selection criteria prioritized peer-reviewed clinical studies with defined sample sizes, FDA documentation for approved medications, and data from recognized medical research institutions.
We included studies from 2006-2026, with an emphasis on research published in 2024-2026 that reflects the most current understanding of GLP-1s and perimenopause.
Limitations of this guide include the following.
- Most peptide clinical trials do not stratify results by menopausal status, which means perimenopause-specific efficacy data is limited.
- Growth hormone peptide research relies heavily on preclinical (animal) studies and small human samples.
- The Mayo Clinic tirzepatide + HRT study was observational with 120 participants, not a randomized controlled trial. Pricing data varies by region, provider, and insurance coverage and changes frequently.
This guide does not constitute medical advice. All peptide therapy decisions should involve a qualified healthcare provider who evaluates your individual health profile.
Citations
- [1] Jastreboff, A.M., et al. (2024). “Tirzepatide Once Weekly for the Treatment of Obesity”. New England Journal of Medicine. PMC10714284.
- [2] Castaneda, R., et al. (2026). “The role of menopause hormone therapy in modulating tirzepatide outcomes”. The Lancet Obstetrics, Gynaecology, & Women’s Health. January 22, 2026.
- [3] Frias, J.P., et al. (2021). “Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes”. New England Journal of Medicine, 385, 503-515.
- [4] Wilding, J.P.H., et al. (2021). “Once-Weekly Semaglutide in Adults with Overweight or Obesity”. New England Journal of Medicine, 384, 989-1002.
- [5] Khera, R., et al. (2016). “Association of Pharmacological Treatments for Obesity With Weight Loss and Adverse Events”. JAMA, 315(22), 2424-2434.
- [6] Falutz, J., et al. (2010). “Effects of tesamorelin in HIV-infected patients with abdominal fat accumulation”. Journal of Acquired Immune Deficiency Syndrome, 53(3), 311-322.
- [7] Chihara, K., et al. (2006). “Efficacy and safety of growth hormone in adult Japanese patients with GH deficiency”. Growth Hormone & IGF Research, 16(2), 132-142.
- [8] Mauvais-Jarvis, F., et al. (2013). “The role of estrogens in control of energy balance and glucose homeostasis.” Endocrine Reviews, 34(3), 309-338.
- [9] Davis, S.R., et al. (2012). “Understanding weight gain at menopause.” Climacteric, 15(5), 419-429.
- [10] Epel, E.S., et al. (2000). “Stress and body shape: stress-induced cortisol secretion is consistently greater among women with central fat.” Psychosomatic Medicine, 62(5), 623-632.
- [11] Iranmanesh, A., et al. (1991). “Age and relative adiposity are specific negative determinants of the frequency and amplitude of growth hormone secretory bursts.” Journal of Clinical Endocrinology & Metabolism, 73(5), 1081-1088.
- [12] Mitchell, W.K., et al. (2012). “Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength.” Frontiers in Physiology, 3, 260.
- [13] Redman, L.M., et al. (2009). “Metabolic and behavioral compensations in response to caloric restriction.” Psychoneuroendocrinology, 34(10), 1012-1018.
- [14] Forbes, J. & Krishnamurthy, K. (2023). “Biochemistry, Peptide”. StatPearls.
- [15] Muller, T.D., et al. (2019). “Glucagon-like peptide 1 (GLP-1)”. Molecular Metabolism, 30, 72-130.
- [16] Cleveland Clinic. (2022). “Human Growth Hormone (HGH)”. Cleveland Clinic.
- [17] Rodriguez, P.J., et al. (2024). “Semaglutide vs Tirzepatide for Weight Loss in Adults with Overweight or Obesity”. JAMA Internal Medicine, 184(9), 1056-1064.
- [18] FDA. (2023). “Zepbound (tirzepatide) Prescribing Information”. U.S. Food and Drug Administration.
- [19] Rubino, D.M., et al. (2022). “Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight”. JAMA, 327(2), 138-150.
- [20] Innerbody Research. (2026). “Best Peptides for Weight Loss”. Innerbody.com. January 18, 2026.
- [21] Zou, P., et al. (2021). “Impact of injection sites on clinical pharmacokinetics of subcutaneously administered peptides.” Journal of Controlled Release, 336, 310-321.
- [22] Renukuntla, J., et al. (2013). “Approaches for enhancing oral bioavailability of peptides and proteins”. International Journal of Pharmaceutics, 447, 75-93.
- [23] Adrian, S., et al. (2019). “Tesamorelin decreases muscle fat and increases muscle area in adults with HIV”. The Journal of Frailty & Aging, 8(3), 154-159.
- [24] Teichman, S.L., et al. (2006). “Prolonged stimulation of growth hormone and insulin-like growth factor I secretion by CJC-1295”. Journal of Clinical Endocrinology & Metabolism, 91(3), 799-805.
- [25] Raun, K., et al. (1998). “Ipamorelin, the first selective growth hormone secretagogue.” European Journal of Endocrinology, 139(5), 552-561.
- [26] Pollak, M. (2004). “Mechanisms by which IGF-I may promote cancer”. Cancer Biology & Therapy, 3(4), S1-S7.
- [27] Sikiric, P., et al. (2013). “Toxicity by NSAIDs: Counteraction by stable gastric pentadecapeptide BPC 157.” Current Pharmaceutical Design, 19(1), 76-83.
- [28] FDA. (2023). “Certain Bulk Drug Substances Used in Compounding”. U.S. Food and Drug Administration.
- [29] Chang, C.H., et al. (2017). “Therapeutic potential of pro-angiogenic BPC157 is associated with VEGFR2 activation.” Journal of Molecular Medicine, 95(3), 323-333.
- [30] Badenhorst, T., et al. (2016). “Effects of GHK-Cu on MMP and TIMP expression, collagen and elastin production, and facial wrinkle parameters.” Journal of Aging Science, 4, 166.
- [31] Endocrine Society. (2025). “Combination of obesity medication tirzepatide and menopause hormone therapy results in greater weight loss”. ENDO 2025 Press Release. July 12, 2025.
- [32] Jacobs, B., et al. (2025). “Discontinuation rates of GLP-1 receptor agonists in clinical practice.” Referenced in RAND commentary. PMID: 39888616.
- [33] RAND Corporation. (2025). “GLP-1 Agonists in Perimenopause: Unique Risks and Potential Opportunities”. August 6, 2025.
- [34] Puhl, R.M., et al. (2022). “Psychological impacts of weight regain.” Referenced in RAND commentary. PMID: 35061154.
- [35] Chae, W., Kim, H., & Kim, S. (2015). “Growth hormone treatment and risk of malignancy”. Korean Journal of Pediatrics, 58(2), 41-46.
- [36] FDA. (2023). “Wegovy (semaglutide) Prescribing Information”. U.S. Food and Drug Administration.
- [37] FDA. (2024). “FDA’s Concerns with Unapproved GLP-1 Drugs Used for Weight Loss”. U.S. Food and Drug Administration.
- [38] Bonza, S. (2025). “Peptides in Perimenopause: A Physician’s Cautiously Curious Perspective”. BonzaHealth.com.